
Mildly overweight, middle aged person.
Presenting with bilateral swollen legs. Erythematous and tender.
Negative formal LL Doppler (No DVT’s)
Represents as only minimally responsive to antibiotics – swelling persistant.
On further history, pt had intermittent bilat LL swelling over past 6 months, worse at the end of the day. Getting worse over past ‘weeks’. From being completely well, to having difficulty climbing a flight of stairs over the course of a year. Gradually worsening SOBOE.
No meds. No PMHx other than “hole in heart” fixed at 1yo in London.
Thoughts?
Well, bilateral cellulitis is exceedingly rare in ambulant non-immunocompromised well adults with no PMHx.
Bloods: CRP 10, WCC wnl. otherwise normal. Troponin negative.
ECG New AF w rate ~80.
Obs wnl, afebrile. Pitting oedema to mid thigh. Erythematous legs. Mildly tender on deep palpation. Not warm.
CXR:

…Formally reported as normal.
Bedside ultrasound was performed:
That left atrium looks big. Sometimes an off angle PLAX slice can make the LA look bigger than it truly is. However note that this slice seems reasonable in that it is on axis, and both the MV and AV are visible. In practice I actually checked my probe positioning and tried a rib space higher as well.
The classic D sign, indicative of R heart strain. Note the RV looks big as well – it’s not normally that prominent at the level of the papilla.
Apical views are notorious for exaggerating the size of atria depending on how the slice cuts through the patient. However, this view is on axis (probe at apex). That was the largest I could get the LA to appear. Even then the RA looks very enlarged (it’s usually smaller than the LA). During diastole (MV snaps open), note how the atrial septum pushes into the LA. That suggests some serious right heart strain.
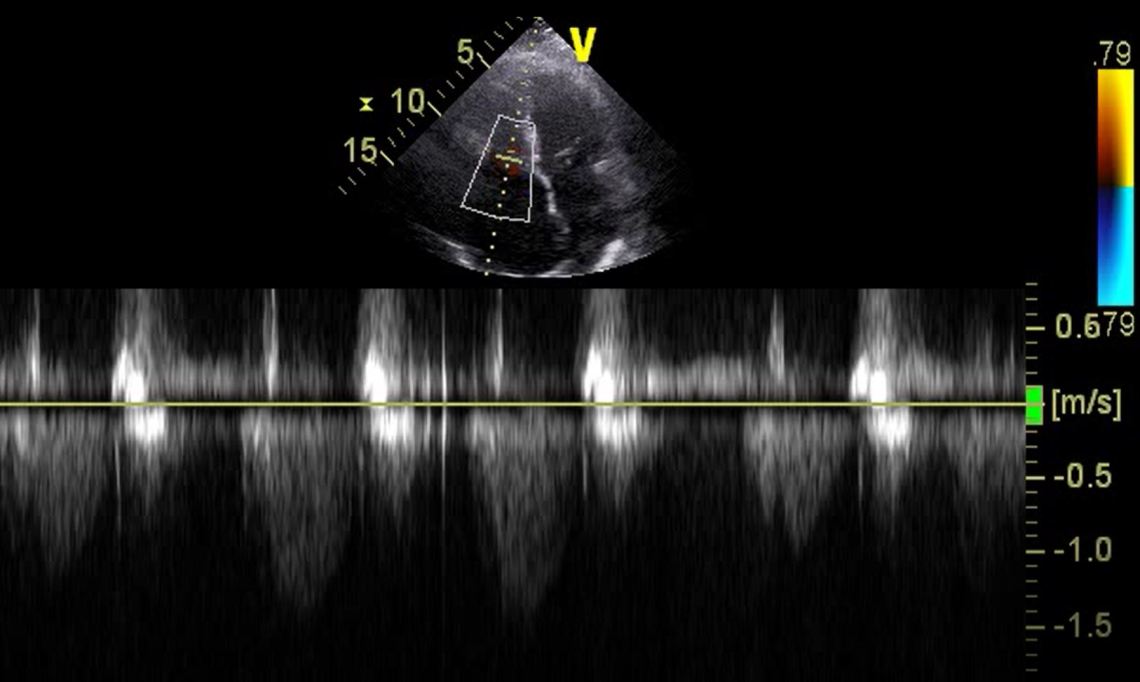
Doing what anyone would do – a TR Max Velocity. It’s >3 in PHTN. However, due to the patient’s body habitus, the image was suboptimal, and it’s difficult to determine where the true TR Jet envelope really lies on CWD. You could seriously underestimate TR VMax when the CWD is not placed in the TR Jet. It’s very unlikely this patient’s TRVMax is less than 1.5 as suggested by the image above. This is why cardiac sonographers will always try to corroborate findings on two views.
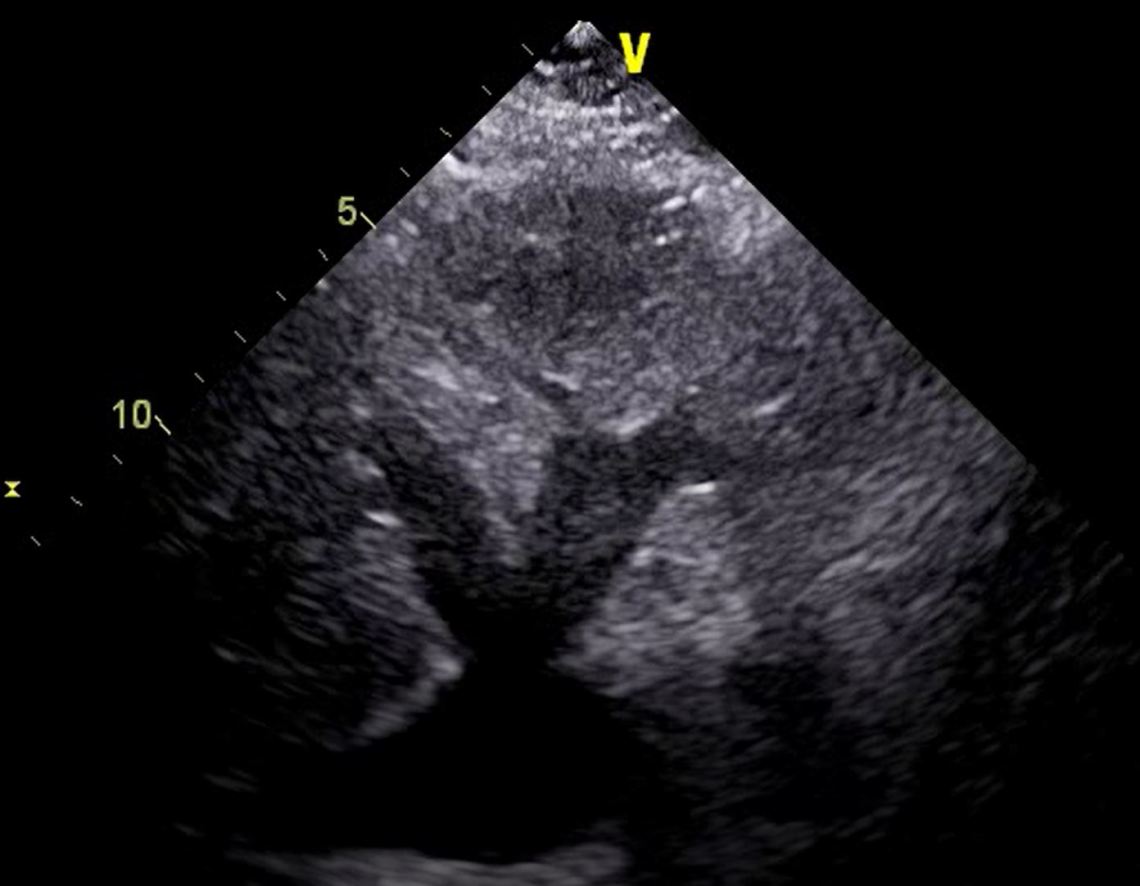
You cannot overestimate the size of the RA on a subcostal window.
This patient had a gastric bubble overlying zis heart, and this view was obtained with difficulty. The RA was obviously enlarged.
Mild ascites (splenorenal space shown) and mild bilateral pleural effusions are seen. POCUS is much more sensitive for effusions than CXRs.
Impression: Right Heart Failure/Strain w new AF.
Plan / Disposition:
CTPA to rule out Pulmonary Embolism.
Empiric Tx for Pulmonary Embolism until CTPA negative.
Referral to cardiology for formal TTE and treatment.
Lesson:
Bilateral cellulitis is quite rare in well adults.
Dont forget about PE’s, even with a negative LL Doppler US.
POCUS is more sensitive for pleural effusions.
POCUS can be very misleading if images are off plane! (TRVMax here was <2, which is almost certainly an underestimate)
